Positive final results in stroke
| Melbourne, Australia, 4 May 2022 | ASX: XETRA-DAX: Level 1 ADR: |
CUV UR9 CLVLY |
Executive Summary
- afamelanotide evaluated as safe in mild to moderate arterial ischaemic stroke (NIHSS 1–15, n=6)
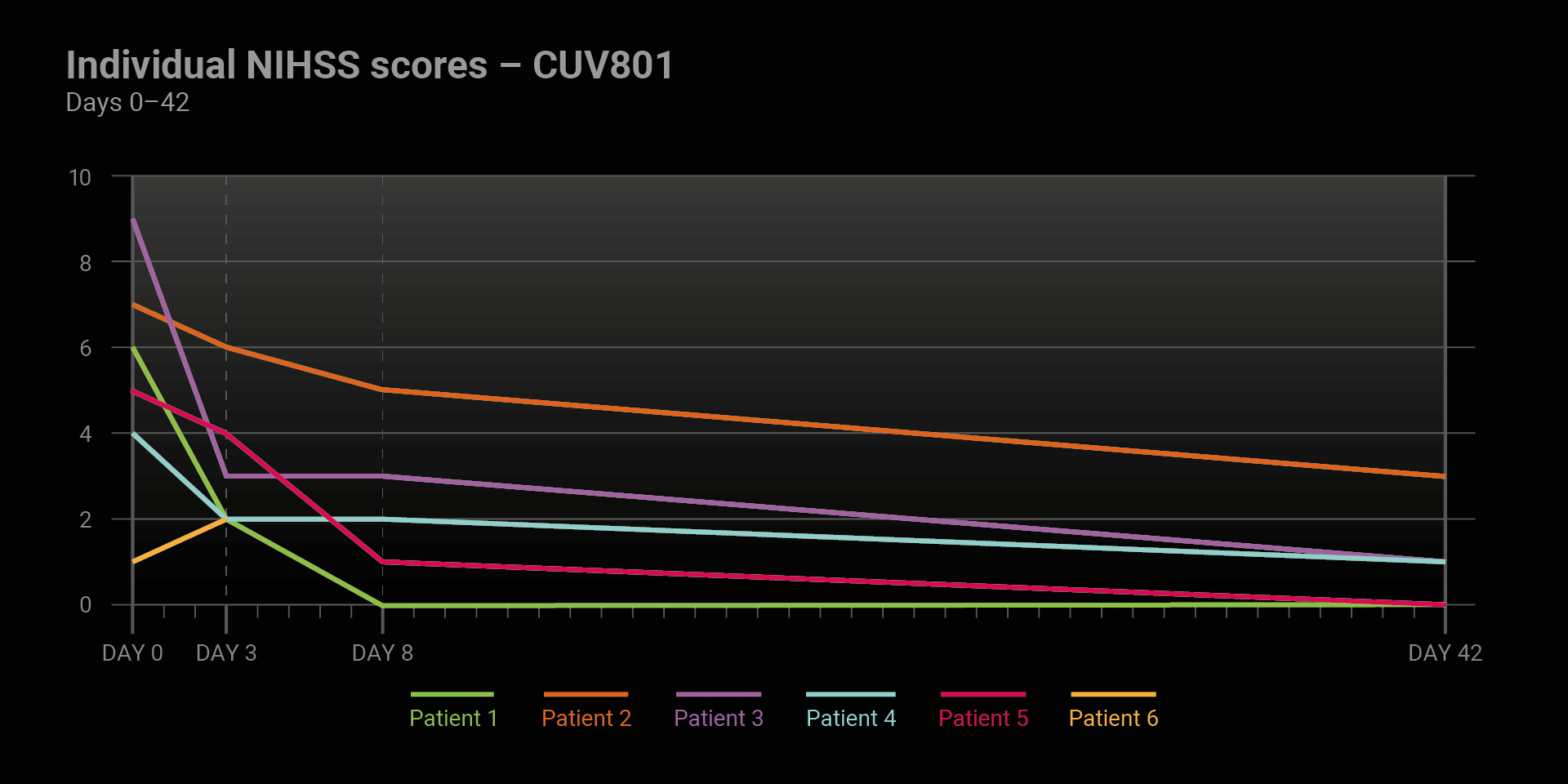
- NIHSS1 scores improved in five patients
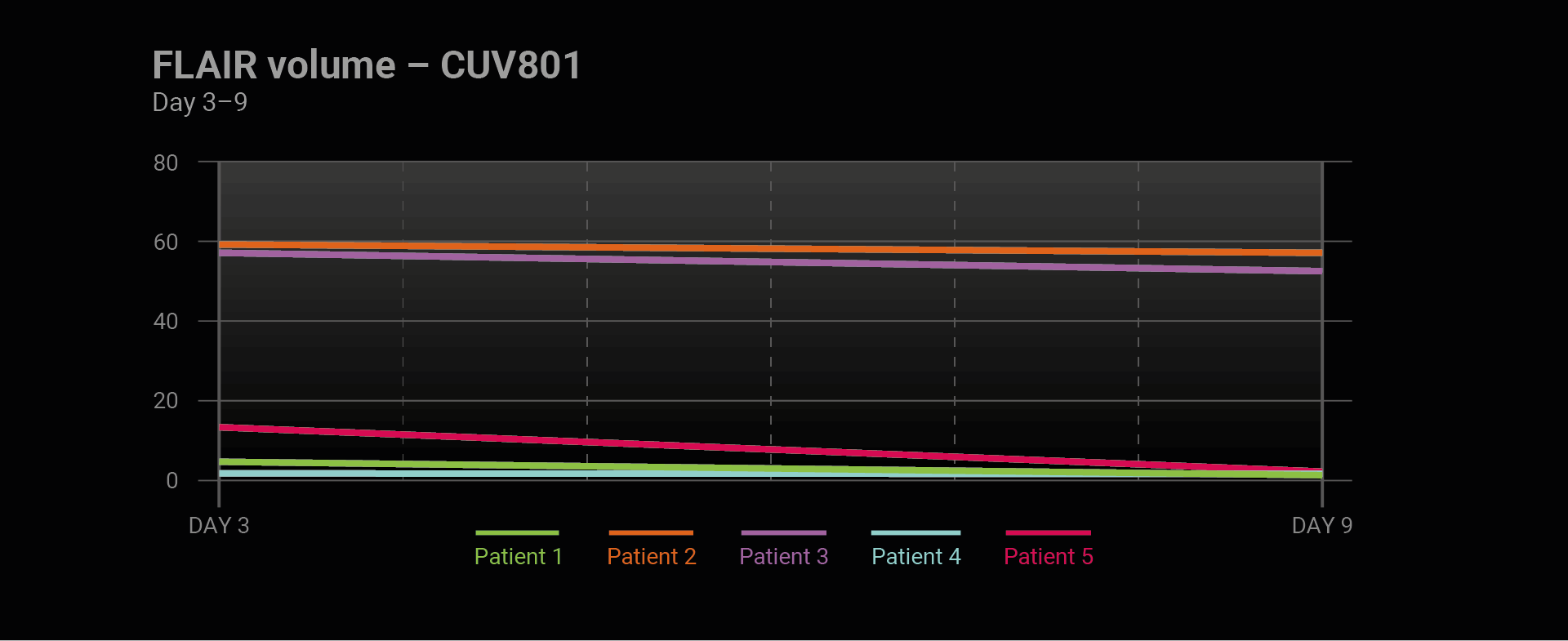
- brain scans (MRI-FLAIR2) in all patients show reduction of affected tissue
- strong functional recovery in all five surviving patients
CLINUVEL today released positive final results of the open label pilot study (CUV801) in arterial ischemic stroke (AIS), evaluating multiple doses of CLINUVEL’s drug afamelanotide in six adult patients. Afamelanotide was shown to be well tolerated, with five of the six patients showing considerable clinical and functional recovery up to 42 days after treatment.
“Final analyses from the CUV801 study show that surviving patients who received treatment with afamelanotide all seemed to have recovered well in the six weeks following their brain injury,” CLINUVEL’s Head of Clinical Operations, Dr Pilar Bilbao said. “Our clinical team often publicly emphasise the significance of afamelanotide as a safe drug in patients, and in this study, we obtained further data that patients with longstanding cardiovascular disease seem to tolerate afamelanotide well. The significance of these findings is of benefit to all our current and future programs.”
Study Results CUV801
CUV801 is the first clinical study assessing afamelanotide as a treatment for a life-threatening brain injury.
All six patients enrolled in the study carried an increased risk of stroke due to their history of cardiovascular disease, elevated blood pressure or diabetes type II, and all suffered a stroke (blood clot) in the left half of the brain. The study was conducted at the specialist stroke unit of the Alfred Hospital in Melbourne, Australia.
Safety was the primary endpoint of the pilot study with afamelanotide administered up to four times over ten days following the stroke. This frequency of dosing seemed not to affect patient safety, with no drug-related adverse events reported during or after the study completion. One patient with a complex cardiovascular history passed away following a second stroke on day 5, which was assessed as unrelated to afamelanotide treatment.
Treatment efficacy was measured using computer imaging to assess the volume of the area affected by the stroke, and validated clinical assessments of function, neurological impairment, and disability.
Analyses of the brain scans (MRI-FLAIR2) performed at days 3 and 9 showed a reduction in size of the affected area in five of the six patients.

Analyses of the NIHSS scores1 up to day 42 indicated that all five surviving patients showed an improvement in neurological functions and reduction in overall impairment (p=0.0625). Four out of five surviving patients showed an improvement of 4 points or more on the scale, regarded as significant, and all five patients reported a clinically meaningful reduction of 3 points. Two patients were symptom free at day 42.
The modified Rankin Scale, a non-stroke specific tool used to determine global disability, proved not sensitive enough as an instrument for the short study period.
Addressing Unmet Medical Need in Stroke
Ischaemic strokes account for around 85% of the estimated 15 million strokes suffered worldwide each year. Stroke is the leading cause of serious, long-term disability in the United States. Considering the staggering prevalence of stroke, the burden of post-stroke recovery and ongoing disability is of primary public health importance.
“Despite the considerable impact of strokes on individuals and society, the treatment options available, even at specialist stroke units, are tragically limited,” Dr Bilbao said. “We are seeking to prove that afamelanotide can provide a safe, effective treatment option which can improve the overall prognosis post-stroke and reduce patient disability long-term.”
“The first steps are to gain comfort that the intervention with afamelanotide poses no harm to patients, while obtaining objective measures of impact of treatment on the course of the patients’ disease. With CUV801 we have achieved both these outcomes and can now pursue further studies and regulatory interactions with a degree of confidence that the drug performs as expected.”
“The gain for stroke patients, but also for society as a whole, lies in the improvement in neurological functions, since the ability to resume independent living saves high costs to our healthcare systems,” Dr Bilbao said.
– End –
- The National Institutes of Health Stroke Scale (NIHSS) consists of 15 tests to evaluate neurologic functioning and impairment caused by acute cerebral infarction (stroke). A clinical assessment is made on the basis of consciousness, language, neglect, visual-field loss, extraocular movement, motor strength, muscle control, speech, and sensory loss. A trained clinician assesses the patient’s ability to answer questions and perform specific activities. In general, the evaluation is made in less than 10 minutes.
- The standard diagnosis of stroke patients is made upon hospital admission through computed tomography perfusion (CTP) images to assess the brain damage caused by the clot. The CTP holds some predictive value to assess whether further brain damage will occur if the clot persists. However, days after the stroke, brain scans are made by magnetic resonance (MRI-FLAIR) providing actual information on the extent of brain damage and recovery.
Appendix I: CUV801 Study Design and Endpoints
The primary objective of the study CUV801 was to evaluate the safety of patients, who were first time administered afamelanotide within 24 hours of suffering a stroke, while a secondary assessment was made of the recovery of brain tissue calculated from the volume of area affected, neurological function assessments and of the overall disability over 42 days.
Validated evaluations were made using:
- National Institutes of Health Stroke Scale (NIHSS)
Evaluation of the patients’ condition through functional assessment on days 0, 1, 2, 3, 4, 7, 8 and 42. - Brain scans
Brain scans (CTP and MRI-FLAIR) were made at various time intervals (day 0, 3, 9) to assess dead brain tissue and areas at risk of irreversible damage, due to an arterial clot. - Evaluation of disability was made using the modified Rankin Scale (mRS) (pre-stroke assessment on day 0, post-stroke assessment on days 7 and 42).
Appendix II: Afamelanotide in Stroke
Scientific progress has demonstrated melanocortins, including afamelanotide, provide a positive effect on the central nervous system (CNS). Afamelanotide is known to offer neuroprotection and act as a potent anti-oxidative hormone. The drug possesses further therapeutic benefits, activating vessels, reducing fluid formation, protecting critical nerve and brain tissue, and restoring the blood brain barrier (BBB: a critical defence mechanism protecting the brain). The drug therapy is thought to improve blood flow and increase the delivery of oxygen and nutrients to deprived brain tissue.
About CLINUVEL PHARMACEUTICALS LIMITED
CLINUVEL (ASX: CUV; ADR LEVEL 1: CLVLY; XETRA-DAX: UR9) is a global specialty pharmaceutical group focused on developing and commercialising treatments for patients with genetic, metabolic, systemic, and life-threatening, acute disorders, as well as healthcare solutions for the general population. As pioneers in photomedicine and the family of melanocortin peptides, CLINUVEL’s research and development has led to innovative treatments for patient populations with a clinical need for systemic photoprotection, DNA repair, repigmentation and acute or life-threatening conditions who lack alternatives.
CLINUVEL’s lead therapy, SCENESSE® (afamelanotide 16mg), is approved for commercial distribution in Europe, the USA, Israel and Australia as the world’s first systemic photoprotective drug for the prevention of phototoxicity (anaphylactoid reactions and burns) in adult patients with erythropoietic protoporphyria (EPP). Headquartered in Melbourne, Australia, CLINUVEL has operations in Europe, Singapore and the USA. For more information, please go to https://www.clinuvel.com.
SCENESSE®, PRÉNUMBRA®, and NEURACTHEL® are registered trademarks of CLINUVEL.
Authorised for ASX release by the Board of Directors of CLINUVEL PHARMACEUTICALS LTD
Media Enquiries
Monsoon Communications
Mr Rudi Michelson, 61 411 402 737, rudim@monsoon.com.au
Head of Investor Relations
Mr Malcolm Bull, CLINUVEL PHARMACEUTICALS LTD
Investor Enquiries
https://www.clinuvel.com/investors/contact-us
Forward-Looking Statements
This release contains forward-looking statements, which reflect the current beliefs and expectations of CLINUVEL’s management. Statements may involve a number of known and unknown risks that could cause our future results, performance or achievements to differ significantly from those expressed or implied by such forward-looking statements. Important factors that could cause or contribute to such differences include risks relating to: our ability to develop and commercialise pharmaceutical products; the COVID-19 pandemic and/or other world, regional or national events affecting the supply chain for a protracted period of time, including our ability to develop, manufacture, market and sell biopharmaceutical products; competition for our products, especially SCENESSE® (afamelanotide 16mg), PRÉNUMBRA® or NEURACTHEL®; our ability to achieve expected safety and efficacy results in a timely manner through our innovative R&D efforts; the effectiveness of our patents and other protections for innovative products, particularly in view of national and regional variations in patent laws; our potential exposure to product liability claims to the extent not covered by insurance; increased government scrutiny in either Australia, the U.S., Europe, Israel, China and Japan of our agreements with third parties and suppliers; our exposure to currency fluctuations and restrictions as well as credit risks; the effects of reforms in healthcare regulation and pharmaceutical pricing and reimbursement; that the Company may incur unexpected delays in the outsourced manufacturing of SCENESSE®, PRÉNUMBRA® or NEURACTHEL® which may lead to it being unable to supply its commercial markets and/or clinical trial programs; any failures to comply with any government payment system (i.e. Medicare) reporting and payment obligations; uncertainties surrounding the legislative and regulatory pathways for the registration and approval of biotechnology and consumer based products; decisions by regulatory authorities regarding approval of our products as well as their decisions regarding label claims; our ability to retain or attract key personnel and managerial talent; the impact of broader change within the pharmaceutical industry and related industries; potential changes to tax liabilities or legislation; environmental risks; and other factors that have been discussed in our 2021 Annual Report. Forward-looking statements speak only as of the date on which they are made, and the Company undertakes no obligation, outside of those required under applicable laws or relevant listing rules of the Australian Securities Exchange, to update or revise any forward-looking statement, whether as a result of new information, future events or otherwise. More information on preliminary and uncertain forecasts and estimates is available on request, whereby it is stated that past performance is not an indicator of future performance.
www.clinuvel.com
Level 11, 535 Bourke Street, Melbourne, Victoria, Australia, 3000, T +61 3 9660 4900, F +61 3 9660 4909